ECR 2015 / C-1903
Radiology of ribs: Spectrum of normal variants and pathological conditions - Emphasis on chest radiograph.
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2015
Poster Number:
C-1903
Type:
Educational Exhibit
Keywords:
Metabolic disorders, Cancer, Education, Cost-effectiveness, Computer Applications-3D, MR, CT, Conventional radiography, Thorax, Bones
Authors:
K. Kalidos1, A. Prahladan2, S. M. Koshy1; 1Trivandrum/IN, 2Thiruvananthapuram/IN
DOI:
10.1594/ecr2015/C-1903
.")
Fig. 1:
Type of costal cartilage calcification in male - Peripheral and band like...
.")
Fig. 2:
Type of costal cartilage calcification in female - Centre and appears nodular...
.")
Fig. 3:
Rib companion shadow - Faint soft tissue density that parallels a segment of...
 with C7 transverse process directing inferiorly.")
Fig. 4:
Cervical rib (bilateral) with C7 transverse process directing inferiorly.
 with T1 transverse process directing superiorly.")
Fig. 5:
Hypoplastic first rib (left) with T1 transverse process directing superiorly.
.")
Fig. 6:
Von luschka’s bifurcated rib (arrow).
.")
Fig. 7:
Anteriorly fused left 3rd and 4th ribs(arrow).
.")
Fig. 9:
Short rib(arrow).
 Chest radiograph, (B) CT - Reformatted image showing rib foramen.")
Fig. 8:
Rib foramen (A) Chest radiograph, (B) CT - Reformatted image showing rib...
.")
Fig. 10:
Pseudoarthrosis of left first rib(arrow).

Fig. 11:
Chest radiograph frontal projection showing ribbon ribs in neurofibromatosis.

Fig. 13:
Inferior rib notching.

Fig. 12:
Chest radiograph in osteopetrosis - Diffuse sclerosis of all bones and splayed...
. Rib findings are - absent or fused ribs(arrow).")
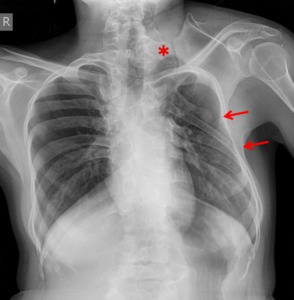
Fig. 14:
Klippel feil syndrome with omovertebral bone (*). Rib findings are - absent or...

Fig. 15:
2 year old child with rickets. Chest radiograph frontal projection shows...
. Note metastatic nodules near right hilum and right subdiaphragmatic region.")
Fig. 16:
Primary hyperparathyroidism: 48 year old man with recurrent disease as...

Fig. 17:
Ollier’s disease. Chest radiograph frontal projection shows multiple...
 Chest radiograph frontal projection shows homogenous opacity involving the right hemithorax with mediastinal shift towards left. Right 2nd rib is not visualized with splaying of adjacent ribs. (B) CT thorax post contrast axial image shows expansile lytic lesion of right 2nd rib with large inhomogenous intrathoracic soft tissue component and spiculated periosteal reaction(arrow). (C) MRI Axial T2WI shows multiple fluid-fluid level in expanded rib and intrathoracic soft tissue component suggestive of secondary ABC changes.")
Fig. 19:
16 year old boy diagnosed as osteosarcoma right 2nd rib with secondary ABC. (A)...

Fig. 18:
Multiple exostosis. Chest radiograph frontal projection shows osteochondromas...
 Chest radiograph frontal projection shows non-homogeneous opacity in left mid and lower zone. Anterior left 5th rib not seperately visualised. (B & C) CT thorax post contrast axial images at soft tissue and bone window. Lytic lesion of left 5th rib with ring and arc type chondroid calcifications of soft tissue component.")
Fig. 21:
Chondrosarcoma rib. (A) Chest radiograph frontal projection shows...

Fig. 20:
Ewings sarcoma. CT thorax post contrast axial images at soft tissue window-...

Fig. 22:
Multiple myeloma. Chest radiograph frontal projection - Expansile lytic lesion...
.")
Fig. 23:
Pancoast tumour. Chest radiograph frontal projections - Irregular opacity in...

Fig. 24:
Chest radiograph frontal projections- Direct erosion of right 3rd and 4th ribs...

Fig. 25:
Chest radiograph frontal projection - Lytic metastasis of left anterior 6th rib...

Fig. 26:
Chest radiograph frontal projection - Expansile lytic metastasis of right 7th...

Fig. 27:
Chest radiograph frontal projection - Sclerotic metastases from carcinoma...

Fig. 28:
Chest radiograph frontal projection - Multiple post traumatic rib fractures on...

Fig. 29:
Chest radiograph frontal projection - Monoostotic fibrous dysplasia of right...

Fig. 30:
Polyostotic fibrous dysplasia. Chest radiograph frontal projection - Expansile...

Fig. 31:
Osteoradionecrosis of left upper ribs. Treated case of left humerus...
 Immediate post op chest radiograph shows resected right 6th rib and residual periosteum. (B) 6 month follow up radiograph shows regrowth and remodeling of right 6th rib.")
Fig. 32:
Post op rib remodeling. Case of Ewing’s sarcoma right 6th rib. (A) Immediate...